Ecomaps allow the therapist to create a snapshot of the social ecology; where the client and family are dislocated. This guides the therapist to understand the impact of intergenerational trauma on belonging, relating, and engaging with people, places, and things in the community. Ultimately, the therapist is to guide the healing to occur within the culture of the family. How can we do this if we don’t understand the context? Therefore, the therapist isn’t the most important resource for the family, they are and their ecosystem is. Elevate the caregivers’ leadership by helping them discover who and what has their back when the emotions get big. Have them decide where they will turn on purpose. Engage the strengths into treatment. Embed the resources into the crisis plan. Work smarter not harder, as a therapist!
Author: Jennifer Benjamin
-
What Reframes Are—and What They Are Not

#ESFT #REFRAMES REFRAMES
In systemic family therapy, reframing is one of the most powerful tools we have. It is also one of the most misunderstood. Too often, reframing is mistaken for persuasion, explanation, or even subtle pressure to “see things differently.” In reality, a reframe is not about convincing anyone to change.
Reframes are not:
- Arguing with caregivers or clients
- Laying breadcrumbs to lead someone to the therapist’s conclusion
- Getting someone to agree with, believe in, or adopt the therapist’s perspective
When reframing turns into persuasion, it loses its power. People don’t change because they are talked into a new idea; they change because something shifts in how they understand the problem.
What a Reframe Actually Is
A reframe offers an alternative lens—one that is relational, developmental, contextual, and trauma informed. It invites caregivers and family members to look at the problem from a different angle, without demanding that they abandon their current understanding.
Rather than saying, “You’re wrong,” a reframe gently asks, “What if this behavior is signaling something else?”
In ESFT, reframes help families move from seeing the problem as:
- The child
- The behavior
- A character flaw or failure
to seeing the problem as:
- An interaction between people
- A pattern shaped over time
- A response rooted in generations, stress, trauma, and context
This shift is subtle—but profound.
From Blame to Pattern
When caregivers view the child as “the problem,” they often feel stuck, frustrated, or powerless. Reframes help caregivers step back and see how everyone in the system is participating in a pattern, often unintentionally. This does not assign blame—it creates possibility.
Suddenly, the behavior is no longer evidence that something is “wrong” with the child. Instead, it becomes a signal that something in the system needs support, structure, or repair.
And when the problem is the pattern, not the person, change becomes possible.
Why Reframes Create Movement
Effective reframes open caregivers’ eyes. They lead to new questions, new emotional responses, and new options for action. Caregivers often find themselves thinking, “I’ve never thought about it that way before.” That moment of curiosity is where change begins.
A reframe doesn’t solve the problem on its own—but it creates the conditions for meaningful work to happen. It prepares the ground for enactment, collaboration, and restructuring.
Because patterns are created together, they can also be changed together—with everyone’s help.
That is the true power of reframing: not convincing people to change, but helping them see that change is possible.
-
January 2026 Newsletter

#image_title We’re excited to welcome you into a new year with our January PCFTTC Newsletter, filled with moments of celebration, growth, and opportunities to stay connected to our learning community.
Inside this issue, you’ll find the launch date for the 3rd Annual MLG Awards, honoring excellence, leadership, and meaningful contributions across our systemic family therapy community. We’re also celebrating a Wickedly Systemic Win showcasing creative and clinically grounded work that brings context to Elphaba’s relationships with her family.
We’re pleased to introduce our new Research Intern, whose work will support PCFTTC’s continued commitment to advancing evidence-informed systemic practice.
You’ll also learn more about The Bridge Program, designed for former trainees who are ready to reconnect and complete their certification journey, the bridge back is open.
Finally, be sure to check out details for our upcoming Free CE Programs on March 11, 2026 & April 22, 2026—an opportunity to growing alongside colleagues in our community.
Thank you for being part of the PCFTTC Alliance. We look forward to another year of collaboration.
To access the NEWSLETTER subscribe to the blog and get the password.
Email Jennifer Benjamin with questions, training@pcfttc.com
-
Agreements for Treatment- Step 1
#image_title The Referral Behavior—Why Naming It Clearly Matters (and Why It’s Not the Problem)
Every course of treatment begins with a referral behavior. A youth is aggressive. A child is refusing school. A caregiver is overwhelmed. A system is worried about safety. These behaviors are the reason therapy begins—but in systemic family therapy, they are not the reason therapy works.
Referral behaviors function as signals, not diagnoses of the system. They tell us where distress is concentrated, not where responsibility lives. When therapists mistake the referral behavior for the problem itself, treatment becomes narrow, reactive, and often ineffective. The family may comply temporarily, but the underlying interactional pattern remains unchanged.
Best practice requires that the referral behavior be named clearly and collaboratively. Families deserve transparency about what brought them into care and how the therapist understands that concern. At the same time, systemic therapists must explicitly distinguish between the presenting behavior and the relational context that gives it meaning.
For example, a child’s aggression may appear to be the primary issue. But aggression rarely exists in isolation. It often emerges within systems struggling with inconsistent caregiver leadership, unresolved trauma, or chronic stressors embedded in the family’s social ecology. Without clarifying this distinction early, families may assume therapy is about “fixing the child,” reinforcing blame and undermining engagement.
Agreements for treatment begin here. Therapists must clearly state:
- What the referral behavior is
- Who noticed the behaviors
- How did we get here
This clarity creates safety. It helps caregivers feel less blamed and more capable. It invites collaboration rather than compliance. It also sets realistic expectations: therapy is not about eliminating a behavior in isolation but about restructuring the relationships that sustain it.
When referral behaviors are framed systemically, families can begin to see the problem as shared rather than owned by one individual. This reframing lays the groundwork for all future agreements about participation, dosage, and responsibility for change.
In short, you cannot form an ethical or effective agreement for treatment unless everyone understands what brought them together—and what that behavior truly represents.
-
The Winner of the Wicked Competition
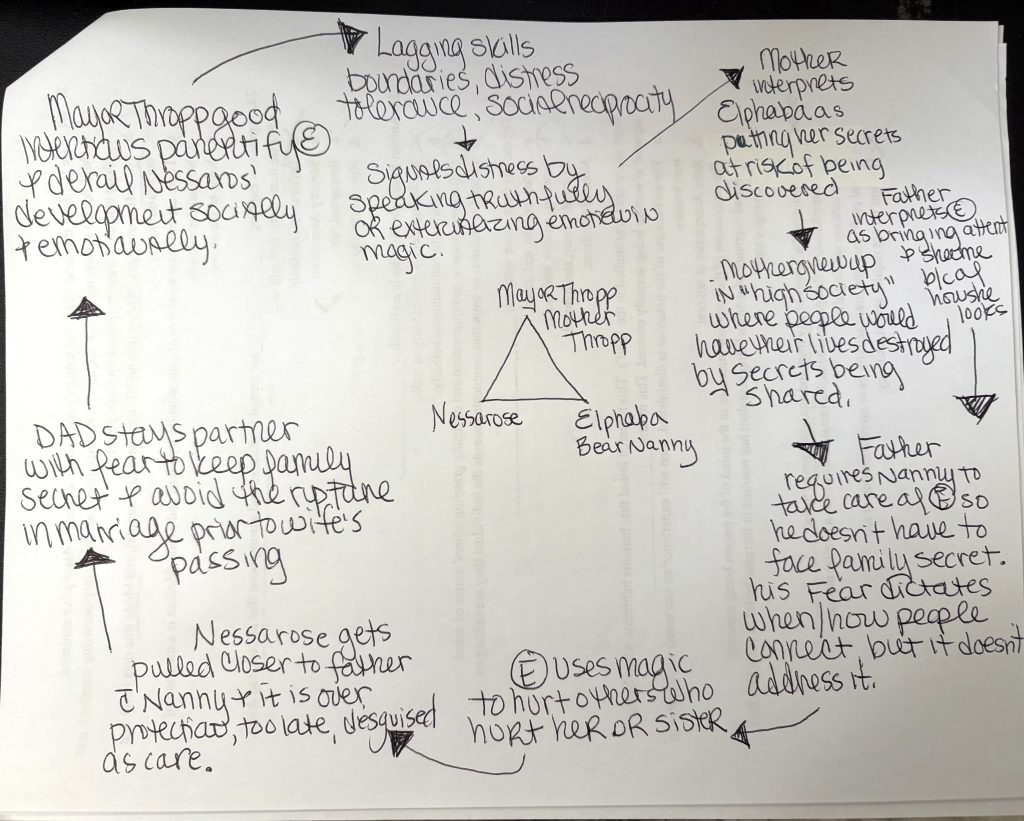
#image_title As part of our Wicked Competition, participants were invited to apply Ecosystemic Structural Family Therapy (ESFT) concepts to the world of Wicked—and one submission stood out for its clarity, creativity, and clinical precision.
The winning entry mapped the family system using both an ecomap and a Negative Interactional Pattern (NIP). Featured here is the NIP, which places Nessarose, Elphaba, the Bear Nanny, Mayor Thropp, and Mrs. Thropp as part of the triangle.
Rather than focusing on individual pathology, the NIP highlights how each person’s responses are relationally organized and mutually reinforcing. Within this triangle, well-intentioned caregiving, protection, and authority intersect in ways that unintentionally intensify disconnection, over-responsibility, and emotional isolation—particularly for Elphaba and Nessarose.
From an ESFT perspective, the NIP illustrates how:
- Caregiver fear and societal pressure shape parental leadership
- Protective behaviors escalate rather than soothe distress
- Children are pulled into roles that strain attachment and emotion regulation
- The broader ecology (including loss, stigma, and power) amplifies family stress
What made this submission especially strong was its ability to show how everyone is doing the best they can within a system that needs support—not blame. The NIP becomes a roadmap for intervention, pointing clinicians toward strengthening leadership, clarifying roles, and shifting interactional sequences rather than “fixing” a single character.
Congratulations to our Wicked Competition winner for reminding us that even in Oz, behavior makes sense in context—and systems, not individuals, are where change begins.
-
The Trauma of Being Unprotected
When Safety and Relationship Collide

#image_title Dec 28, 2025
-
Wicked Characters as Family Systems Metaphors
🌪️ A playful, clinically grounded way to think about family dynamics through the world of Oz
Elphaba — The “Identified Patient” Who Carries the System’s Anxiety
Elphaba represents the youth who is labeled as “the problem” simply because the system doesn’t understand or accommodate their uniqueness.
In ESFT terms, she is the symptom bearer—not because she’s broken, but because her family, community, and social ecology project their fears and failures onto her.
Her journey mirrors the work of helping a child reclaim identity, voice, and relational belonging.
Glinda — The Caregiver Who Uses Performance to Maintain Harmony
Glinda embodies the caregiver (or sibling) who copes through positive affect, charm, and high sociability.
Her role keeps peace but often hides insecurity.
In systemic therapy, she symbolizes the family member whose over-functioning or “performer” role helps stabilize the system—but prevents vulnerability.
Her friendship with Elphaba demonstrates the healing power of authentic connection.
Fiyero — The Avoidant Attachment Partner Afraid to Choose
Fiyero mirrors the person in the system who avoids emotional engagement—“fun,” charming, but disconnected.
He represents a protective adaptation, not a flaw.
Through relationship with both Glinda and Elphaba, he learns the core principles of systemic change:- Responsibility
- Presence
- Emotional risk-taking
The Wizard — The Larger System That Creates the Problem It Claims to Solve
The Wizard symbolizes structural forces—policies, institutions, and leaders—that blame individuals while perpetuating dysfunction.
He is the metaphor for:- Oppressive systems
- Pathologizing narratives
- Blame-shifting structures
In family therapy terms, he is the “macro-system stressor” shaping how families respond to crisis.
Madame Morrible — The Rigid Hierarchy That Reinforces Dysfunction
Morrible represents the family system’s coercive hierarchy—a figure who uses fear, control, and manipulation to maintain order.
Her “weather patterns” metaphorically mirror how emotional climates in families are often shaped by the most powerful or reactive members.
Nessarose — The Child Caught in the Bind of Overprotection
Nessarose is the sibling who receives intense focus—overprotection disguised as care.
Her storyline reflects how enmeshment and over-dependence can limit growth and create resentment, despite good intentions.
Her dynamic with Elphaba shows what happens when families assign fixed roles (“the responsible one,” “the helpless one”).
Boq — The Marginalized Member Who Adapts Until He Breaks
Boq embodies the overlooked, underheard member of the system who tries to earn belonging through compliance.
His unmet needs eventually transform him—literally—revealing how suppressed emotions can reshape functioning.
He is the metaphor for accommodation patterns and role strain.
Dr. Dillamond — The Silenced Voice of Wisdom
Dillamond represents the voice in the system that sees the truth but is ignored or suppressed.
He symbolizes the disenfranchised perspective—the teacher, elder, or natural support whose insight is essential to systemic change, but often marginalized.
Dorothy (Part 2) — The Newcomer Who Exposes Existing Fault Lines
Dorothy is the outsider whose arrival destabilizes a fragile system.
Her presence reveals:- unresolved grief
- fractured alliances
- long-standing injustices
She is the catalyst that forces the system to confront its hidden patterns.